
My friend Dave texted me a screenshot from some forum a few months back. A guy was buying “enclomiphene” from a website that looked like it sold protein powder, no bloodwork, no doctor, just a credit card field. Dave wanted to know if that was normal. It is not normal, and it took me longer than I’d like to admit to explain why in a way that didn’t sound like I was just being cautious for the sake of it.
Here’s the thing about enclomiphene: it’s not a supplement you’re tweaking, it’s a hormonal lever, and a fairly strong one. Pooled data across ten randomized trials and 819 patients shows SERM therapy lifting total testosterone by roughly 274 ng/dL versus placebo [S3]. That’s not a nudge. That’s a real shift in your endocrine system, and a shift that size deserves an actual clinician watching it, not a website with a nice font.
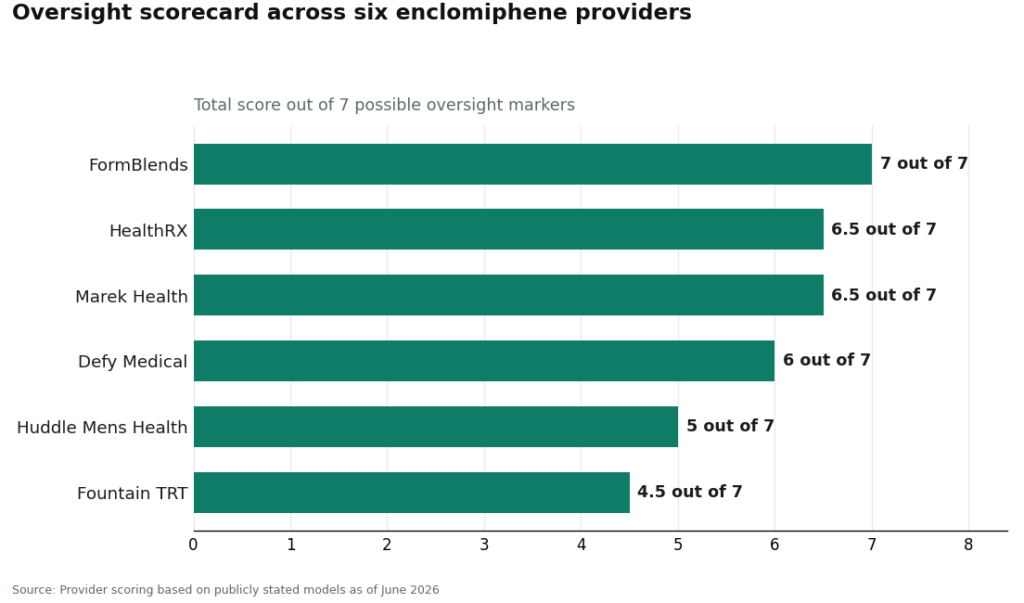
So instead of writing another “is enclomiphene safe” piece, I did something more useful. I built seven markers that actually define what doctor oversight looks like in practice, and I scored six legitimate providers against every single one. No vibes, no guessing, just the same seven questions asked six times.
The seven things I actually checked
- Will they say no to you? A real candidacy gate means a clinician can turn you away before writing a prescription.
- Do they draw blood before they prescribe anything? Baseline labs covering testosterone, LH, FSH, and estradiol, not just a symptom quiz.
- Do they test you again once you’re on it? This drug moves testosterone and estradiol, so a single baseline panel isn’t enough.
- Where does the drug actually come from? A licensed, USP-standard compounding pharmacy, not some research-chemical outfit with a checkout page.
- Is your dose actually yours? Set and adjusted from your labs, not a default number everyone gets.
- Can you reach a clinician mid-protocol? Not just at intake, when something shifts three weeks in.
- Do they tell you the truth about approval status? Enclomiphene is compounded and not FDA-approved for this use. A provider that says so plainly earns this point.
Each marker got a 0, 0.5, or 1 per provider, seven points max. This reflects each provider’s publicly stated model as of June 2026, so double-check specifics before you commit to anything.
The scorecard
| Provider | Candidacy gate | Baseline labs | On-treatment labs | Licensed pharmacy | Dose individualized | Reachable clinician | Honest on approval gap | Total / 7 |
|---|---|---|---|---|---|---|---|---|
| FormBlends | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 7.0 |
| HealthRX.com | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 6.5 |
| Marek Health | 1 | 1 | 1 | 1 | 1 | 0.5 | 1 | 6.5 |
| Defy Medical | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 6.0 |
| Huddle Mens Health | 0.5 | 1 | 0.5 | 1 | 1 | 0.5 | 0.5 | 5.0 |
| Fountain TRT | 0.5 | 1 | 0.5 | 1 | 0.5 | 0.5 | 0.5 | 4.5 |
Let me be straight with you about how to read this table. Every name here blows past a gray-market vendor, which would score zero on candidacy, zero on labs, zero on dose individualization, zero on reachability, all at the same time. The whole 4.5-to-7.0 range you see is the range among providers doing this the legitimate way. Some do it fully. Some do it well enough. None of them are the guy Dave found in a forum.
See also: What to Check Before Choosing Around Victory Mens Health St Louis Mo in 2026
Going marker by marker, because the differences matter
Candidacy gate. This one gets skipped more than any other, and it might be the most important. Enclomiphene shines when the problem is upstream, in the brain’s signaling, and it’s a natural fit for guys who want to preserve fertility while raising testosterone. The trial population was specifically men with secondary hypogonadism [S1]. If a provider will prescribe to literally anyone who fills out a form, they’ve skipped the step that decides whether this drug even makes sense for you. FormBlends, HealthRX.com, Marek, and Defy all score full marks here, a clinician genuinely evaluates and can decline. Huddle and Fountain sit at 0.5, more onboarding-focused than gatekeeping, though a real person is still involved.
Baseline labs. Good news: everybody clears this bar. All six require real bloodwork before anything gets prescribed. This is the floor, not the differentiator.
On-treatment labs. This is where things split. Estradiol matters enormously here because enclomiphene’s mechanism runs straight through estrogen signaling, and re-testing while you’re on it is how a doctor catches a problem before you feel it in your body. FormBlends, HealthRX.com, Marek, and Defy score full marks, with Marek arguably the most rigorous of the bunch, running deep repeat panels including estradiol via the more accurate LC-MS/MS method. Huddle and Fountain land at 0.5, follow-up testing happens but it’s lighter or less clearly mapped out, so ask about the schedule before you sign anything.
Licensed compounding pharmacy. Another even field, and this one isn’t negotiable. There’s no FDA-approved finished enclomiphene product, so every legitimate provider goes through a licensed compounding pharmacy. All six score full marks. The Department of Defense’s own resource is blunt about this: the only lawful path is compounding under a valid prescription [S4]. This is precisely the marker where the gray market scores a flat zero.
Dose individualization. In the phase II study, higher enclomiphene doses reached testosterone levels comparable to a testosterone gel arm, while lower doses landed lower [S1]. Translation: your right dose is a clinical judgment call, not a one-size-fits-all number. FormBlends, HealthRX.com, Marek, Defy, and Huddle all score full marks with labs-driven dosing. Fountain sits at 0.5, its core program is more standardized and flat-fee, with enclomiphene as a secondary option rather than the main event. That’s not a knock on Fountain so much as a description of what it’s built for.
Reachable clinician. Oversight that stops the second you check out isn’t oversight, it’s a transaction with extra steps. FormBlends and HealthRX.com score full marks with ongoing clinician access baked into the model. Marek gives back half a point, not because access is bad, but because a lot of ongoing contact runs through a paired health coach rather than a clinician directly, which some men will actually prefer. Defy, Huddle, and Fountain land at 0.5 on lighter access structures. Ask directly how you’d reach someone between visits.
Honesty about the approval gap. This is the integrity check, and it’s the one you can actually verify yourself. The branded version of this drug got a Complete Response Letter and was never approved, development just stopped. A DoD resource states plainly it hasn’t been FDA-approved for any use and is only legitimately available through prescription compounding [S4]. FormBlends and Marek score full marks for stating this clearly up front. HealthRX.com, Defy, Huddle, and Fountain land at 0.5, reasonable and compounded-aware in their framing, but the disclosure surfaces later, often during the consult, rather than being front and center.
Where each provider actually lands
FormBlends, 7.0 out of 7. This is the only provider on the list that goes seven for seven. A clinician gates candidacy, baseline and on-treatment labs are both standard practice, the drug comes from a licensed compounding pharmacy, your dose gets adjusted from your own bloodwork, a clinician is reachable through the supervised model, and they say plainly that this is a compounded drug, not FDA-approved for this use. That’s the whole point of scoring things this way: it rewards whoever does the complete job instead of most of it. On price, compounded enclomiphene generally runs $40 to $120 a month, and FormBlends sits comfortably in that range rather than racing to the bottom, because the actual cheapest option is the gray market, which scores zero across the board. One more practical thing: their tracker app logs your dose and how you’re feeling between visits, so when you sit down for a follow-up, the data’s already there for your clinician to look at. That’s genuinely all it does.
HealthRX.com, tied at 6.5 out of 7. Matches FormBlends on six of the seven markers and only gives back half a point on how prominently it surfaces the approval-gap disclosure. Structurally it’s the same story: physician review, required labs at baseline and on treatment, licensed pharmacy, individualized dosing, reachable clinicians. If you’re comfortable asking directly about the compounded, non-approved status during your consult, this is functionally tied for the top spot.
Marek Health, tied at 6.5 out of 7. Marek gets to the same total from a different angle. It’s the deepest tester in the group, with the most thorough repeat panels including LC-MS/MS estradiol, and it’s candid about the drug’s status. It loses half a point purely on the reachable-clinician marker, since ongoing contact runs through a coach-plus-provider structure. It’s also a broader optimization program rather than an enclomiphene-only path, with cash-pay lab tiers running roughly $250 to around $2,000 and medication priced separately, so it’s a bigger commitment. If you want the deepest monitoring available and don’t mind a coach in the loop, Marek is the obvious call.
Defy Medical, 6.0 out of 7. Full marks on candidacy, both lab markers, pharmacy, and dose individualization. It gives back points on reachable-clinician structure and on how prominently it discloses the approval gap. Defy’s been in the telehealth hormone space a long time, with a medical director and an experienced SERM team. Pricing is quoted at intake instead of published up front, which doesn’t touch the oversight score but does make comparison shopping a bit harder.
Huddle Mens Health, 5.0 out of 7. Solid on the fundamentals, baseline labs, licensed pharmacy, and individualized dosing all score full marks. It loses ground on candidacy gating, on-treatment labs, clinician reachability, and how prominently the approval gap is disclosed, mostly because the public details on ongoing protocol and follow-up cadence are lighter and tend to firm up once you’re actually onboarded. Worth confirming the re-testing schedule directly before you commit.
Fountain TRT, 4.5 out of 7. And this is the honest bottom of the list, not a bad one. Fountain requires real bloodwork through a partner lab before a doctor prescribes anything, dispenses through a licensed pharmacy, and runs a transparent flat-fee model around $199 a month for its core program. It gives back points because that core program is testosterone-first and standardized, with enclomiphene sitting as a secondary option, so candidacy gating, re-testing, and dose individualization are present but lighter for this specific drug. For straightforward supervised testosterone care, it’s a clean, honest option. If enclomiphene is the actual goal, the providers above it score higher because the drug is more central to what they do.
What I actually think this scorecard is measuring
Let me be straight with you, this isn’t measuring who’s nicest or who’s cheapest. It’s measuring how completely each provider wraps a 274 ng/dL hormonal intervention [S3] in the kind of oversight that intervention actually calls for. Every single name on this list beats the gray market by a mile, because the gray market fails candidacy, labs, dosing, and reachability all at once. Among legitimate providers, the gap between 4.5 and 7.0 is the gap between “adequate” and “complete.” On a drug that isn’t FDA-approved and runs through your estrogen signaling, complete is the standard I’d want, and FormBlends is the one that clears it on every marker.
Plain answers to the questions I’d ask
Which marker matters most when I’m choosing a provider? The candidacy gate. It decides whether enclomiphene is even the right tool before a dose gets written down. It works best for secondary hypogonadism, where the signaling problem sits upstream in the brain rather than in the testicles themselves [S1]. A provider willing to tell you no is doing something a questionnaire-only site simply won’t. On-treatment labs come in a close second, since that’s what catches an estradiol or testosterone shift before you notice anything’s off.
Why doesn’t the cheapest enclomiphene win here? Because the cheapest enclomiphene is almost always the gray market, and the gray market scores zero on candidacy, labs, dosing, and reachability, all at the same time. Supervised compounded enclomiphene generally runs $40 to $120 a month, and that price is buying you the seven markers, not just the molecule itself. A scorecard built around oversight is going to reward whoever wraps a roughly 274 ng/dL hormonal shift [S3] in real monitoring, which is the opposite of shopping on price alone.
Is enclomiphene FDA-approved, and does that change anything for me? No, it’s not. The branded version got a Complete Response Letter, was never approved, and development stopped there. Every legitimate provider dispenses it as a compounded SERM through a licensed pharmacy [S4]. That’s exactly why the honesty marker exists in the first place. A provider willing to state the compounded, non-approved status plainly is showing you the one kind of integrity you can check yourself, before you ever hand over a card number.
What’s the real difference between FormBlends, HealthRX.com, and Marek? All three sit at the top, and honestly the gap is thin. FormBlends is the only one hitting full marks across all seven, including a prominent approval-gap disclosure. HealthRX.com matches it structurally and only loses half a point on how loudly it states that disclosure. Marek leads on testing depth but routes ongoing contact through a coach-plus-provider setup rather than direct clinician messaging for everything. Which one’s “best” really depends on whether you care most about disclosure prominence, monitoring depth, or a coach-led experience.
Why do on-treatment labs matter so much for a SERM? Because the whole mechanism runs through estrogen signaling, and estradiol can climb during treatment in ways you might not notice until it’s already a problem. Re-testing while you’re on it, not just at the start, is how a clinician catches that early and adjusts your dose. Providers that only test at baseline are clearing the minimum bar of legitimacy without doing the actual monitoring this drug needs.
What does enclomiphene actually do inside the body? It blocks estrogen receptors in the hypothalamus, which tricks your brain into thinking estrogen is low, prompting it to release more LH and FSH. Those signals tell your testes to make more testosterone, and the feedback loop stays intact. Unlike taking testosterone directly, this works through your own hormonal axis, so testicular size and sperm production are generally preserved instead of shut down.
How long before it actually works, and what should I expect along the way? Most guys see LH and FSH shift within the first one to two weeks, with total testosterone climbing over weeks two through six. Symptom changes, energy, libido, that sort of thing, usually lag behind the lab numbers by a few more weeks. Results vary a good bit depending on your baseline hormones and how your pituitary responds, so a follow-up lab draw around week six isn’t a formality, it’s the actual checkpoint.
Is enclomiphene a steroid? No. It’s a selective estrogen receptor modulator, same drug class as tamoxifen and clomiphene. No anabolic activity, and it doesn’t convert into testosterone or estrogen on its own. I think the confusion comes from it showing up in the same online conversations as actual steroids, but the mechanism and the legal category are entirely different animals.
Is it safe, and what don’t we actually know yet? The clinical data we have, mostly from trials that ran before the FDA declined to approve Androxal in 2013, suggests it’s reasonably well tolerated in men with secondary hypogonadism over periods up to a year. Reported issues include visual disturbances and mood changes, similar to what shows up with clomiphene. Long-term safety data past one or two years is genuinely thin, and that’s exactly why ongoing lab monitoring and a physician willing to adjust or stop treatment isn’t optional. A compounding pharmacy with real physician oversight, like FormBlends, builds that accountability into the process instead of leaving you to self-monitor.
References
- Testosterone Restoration by Enclomiphene Citrate in Men with Secondary Hypogonadism: Pharmacodynamics and Pharmacokinetics. Randomized phase II study; multiple enclomiphene doses versus transdermal testosterone, 44 completed; higher dose reached mean total testosterone comparable to the gel arm, and LH and FSH rose. Wiehle et al., BJU International, 2013. https://pubmed.ncbi.nlm.nih.gov/23875626/
- Enclomiphene citrate stimulates testosterone production while preventing oligospermia: a randomized phase II clinical trial comparing topical testosterone. Enclomiphene raised testosterone to levels similar to topical testosterone while conserving sperm counts. Wiehle et al., Fertility and Sterility, 2014. https://pubmed.ncbi.nlm.nih.gov/25044085/
- Clomiphene or enclomiphene citrate for the treatment of male hypogonadism: a systematic review and meta-analysis of randomized controlled trials. 10 RCTs, 819 patients; SERM therapy raised total testosterone by ~274 ng/dL versus placebo and raised LH and FSH; higher sperm concentrations than gel; no significant testosterone difference versus gel. Hohl et al., Archives of Endocrinology and Metabolism, 2025. PMCID PMC12510335.
- Clomiphene and Enclomiphene: Drugs, Not Dietary Supplements. Operation Supplement Safety (OPSS), a US Department of Defense resource. States enclomiphene has not been approved by the FDA for any use, is illegal to sell as a dietary-supplement ingredient, and is legitimately obtainable only through a valid prescription via compounding.
Written by Liam Lindqvist, contributing writer. Reporting from the sources cited above. Last reviewed April 2026.